AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2640-1053/082
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Manchester, M8 5RB, United Kingdom.
Citation: Anthony Kodzo-Grey Venyo. (2021) Signet Ring Cell Carcinoma of the Prostate Gland: A Review and Update. Cancer Research and Cellular Therapeutics. 5(3); Doi: 10.31579/2640-1053/082
Copyright: © 2021, Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 April 2021 | Accepted: 07 May 2021 | Published: 11 June 2021
Keywords: signet-ring cell carcinoma; prostate; primary; metastatic; biopsy; ultrasound scan, computed tomography scan; histopathology; immunohistochemistry; PSA; AE1/AE3. CAM; Ki-67; PAS-diastase; mucicarmine; alcian blue;
Signet-ring cell carcinoma of the prostate gland (SRCCP) an uncommon and aggressive malignant tumour of the prostate gland which is characterized by histopathology examination features of compression of the nucleus into the form of a crescent by a large cytoplasmic vacuole. SRCCPs that have so far been reported have been either (a) primary tumours, metastatic tumours with the primary tumour elsewhere with the gastro-intestinal tract being the site of the primary tumour but the primary tumour could originate elsewhere, and additionally some reported SRCCPs have been classified as carcinoma of unknown primary. SRCCP could be a pure tumour or a tumour that is contemporaneously associated with other types of tumour including various variants of adenocarcinoma. SRCCP can manifest in various ways including: Incidental finding following prostatectomy that has been undertaken for a presumed benign prostatic hyperplasia, lower urinary tract symptoms, visible and non-visible haematuria, raised levels of serum PSA but some SRCCPs have been diagnosed with normal / low levels of serum PSA, there may be a history of dyspepsia in cases of metastatic signet-ring cell carcinoma in association with contemporaneous primary signet-ring cell carcinoma of the stomach or there may be a past history of surgical treatment for signet-ring cell carcinoma of the gastrointestinal tract, or bleeding from the gastrointestinal tract in cases of upper gastrointestinal tract and rectal bleeding as well as change in bowel habit for primary tumours of the anorectal region, retention of urine, and rarely a rectal mass in the case of SRCCP with an anorectal primary tumour. In order to exclude a primary signet ring cell carcinoma elsewhere, a detailed past medical history is required as well as radiology imaging including contrast – enhanced computed tomography (CECT) scan and contrast-enhanced magnetic resonance imaging (CEMRI) scan as well as upper gastrointestinal endoscopy and colonoscopy to exclude a primary lesion within the gastrointestinal tract. Diagnosis of SRCCP requires utilization of the histopathology and immunohistochemistry examination features of prostate biopsy, prostatic chips obtained from trans-urethral resection of prostate specimen or radical prostatectomy specimen. SRCCPs upon immunohistochemistry staining studies tend to show tumour that tend to exhibit positive staining for the following tumour markers as follows: PSA – positive staining for PSA has been variable in some studies, AE1/AE3, CAM 5.2, Ki-67 with a mean of 8%, PAS-diastase, Mucicarmine (50%), Alcian blue (60%), Alpha-methyl-acyl coenzyme A racemase (P504S), and Cytokeratin 5/6. SRCCPs also tend to exhibit negative staining for: Bcl2 (rare positive), and CEA (80%). Traditionally the treatment of Primary Signet-Ring Cell Carcinoma of the Prostate Gland has tended to be similar to the treatment of the traditional adenocarcinoma of the prostate gland which does include: hormonal treatment, radiotherapy, and surgery. Nevertheless, considering that primary SRCCPs and metastatic SRCCPs that have been reported in the literature have generally tended to be associated with an aggressive biological behaviour, even though there is no consensus opinion on the treatment of the disease it would be strongly recommended that these tumours that tend to be associated with rapid progress of the disease and poor survival there is an urgent need to treat all these tumours with aggressive surgery including radical prostatectomy plus adjuvant therapies including: radical radiotherapy, combination chemotherapy, selective prostatic angiography and super-selective embolization of the artery feeding the tumour including intra-arterial infusion of chemotherapy agents directly to the tumour, radiofrequency ablation of the tumour as well as irreversible electroporation of the tumour which should form part of a global multicentre study of various treatment options. With regard to metastatic signet-ring cell carcinomas of the prostate gland with a contemporaneous primary tumour elsewhere the primary tumour should also be treated by radical and complete excision of the primary tumour plus radical surgery and aggressive adjuvant therapy. Considering that SRCCPs have tendered not to respond well to available chemotherapy agents, there is need for urologists, oncologists, and pharmacotherapy research workers to identify new chemotherapy medicaments that would more effectively and safely destroy signet-ring cell tumours in order to improve upon the prognosis.
Warner in 2010 [1] iterated that signet-ring ring is a terminology that is utilized to describe the histopathology examination appearance of a tumour cell which is characterized by compression of the nucleus into the form of a crescent by a large cytoplasmic vacuole [2, 3]. and signet-ring cell carcinomas had been estimated to occur in 2.5% of cases of adenocarcinoma of the prostate gland [4]. Guerin and associates [2] had stipulated that signet-ring cell carcinoma (SRCC) should be classified as a variant of high-grade adenocarcinomas instead of a separate histopathology diagnosis. Warner et al [1]. indicated that in support of the proposition of Guerin et al [2]. signet-ring cell carcinoma (SRCC) often tends to be found in the presence of other high-grade adenocarcinoma of prostate histopathology patterns. Warner et al [1]. additionally iterated that irrespective of histopathology classification of the tumour, the poor prognosis as well as the rarity of signet-ring cell carcinoma (SRCC) of the prostate gland does warrant closer investigation. Warner et al [1]. iterated that even though SRCC tends particularly to be found within the stomach as well as colon, it could also be found within the pancreas, breast, thyroid gland, urinary bladder, and the prostate gland. The review of the English literature by Warner et al [1]. in 2010, did identify only 42 cases of signet-ring cell carcinoma (SRCC) of the prostate gland that had been described in case reports as well as in case series. Warner et al [1]. stated that several studies had listed up to 17 patients; nevertheless, they were not independently reported therefore they could not be reported independently and therefore they could not be included in their analysis. Warner et al [1]. indicated that the establishment of a diagnosis of SRCC of the prostate gland does require histopathology examination of the tissue of the prostate gland, the finding of a negative gastro-intestinal (GI) work-up which does include the4 undertaking of computed tomography (CT) scan of the abdomen, a colonoscopy, esophagogastroduodenoscopy as well as utilization of various stains for the pathology examination of the specimen which do help in the localization of the primary site of the tumour to the prostate gland. Warner et al [1]. iterated that the prognosis of patients who have signet-ring cell carcinoma (SRCC) of the prostate gland is poor, as well as recommendations regarding the treatment of SRCC of the prostate gland are sparse in view of the fact that very few cases of SRCC of the prostate gland had been reported. Considering that some cases of SRCC of the prostate gland have been reported since 2010, there is the possibility that there would be new information related to the diagnosis, management, and biological behaviour of the tumour. Additionally, considering that only few cases of SRCC of the prostate gland have been reported in the global literature, there is the likelihood that many clinicians including general practitioners, urologists, pathologists and oncologists may not have ever encountered a case of signet-ring cell carcinoma of the prostate gland (SRCCPG) before and therefore they would not be familiar with the diagnostic features, management and outcome of signet-ring cell carcinoma of the prostate gland (SRCCPG). The ensuing article on signet-ring cell carcinoma of the prostate gland (SRCCPG) has been divided into two parts: (A) Overview and (B) Miscellaneous narrations and discussions from case reports, case series, and studies related to signet-ring cell carcinoma of the prostate gland.
To review and update the literature on signet ring cell carcinoma of the prostate gland.
Internet data bases were searched including: Google, Goggle scholar, yahoo, and PUBMED. The search words that were used included: signet-ring cell carcinoma of prostate, prostatic signet-ring cell carcinoma, primary signet-ring cell carcinoma of prostate, metastatic signet-ring cell carcinoma of prostate. Thirty five references were identified which were used to write the review and update on primary and metastatic signet-ring cell carcinoma of the prostate gland which has been divided into two parts: (A) Overview which has discussed various general aspects of signet-ring cell carcinoma in general and of the prostate gland as well as primary and metastatic signet-ring cell carcinoma and (B) Miscellaneous narrations and discussions from some case reports, case series, as well as studies related to primary and metastatic signet-ring cell carcinoma of the prostate gland.
Results / Signet-Ring Cell Carcinoma of the Prostate Gland: Review and Update
[A] Overview
Definition / General Statements on Signet-Ring Cell Carcinomas in General and Signet-Ring Cell Carcinomas of the Prostate Gland.
It has been iterated that primary signet-ring cell carcinoma is a terminology that is utilized for adenocarcinoma of the prostate gland that contains a prominent amount of signet-ring tumour cells [5].
It has been iterated that less than 50 cases of signet-ring cell carcinomas of the prostate gland have been identified within the English literature [6].
It has been documented that signet-ring cell carcinoma of the prostate gland is a highly malignant tumour [6].
With regard to the surgical diagnostic criteria the ensuing summations have been made: [5]
It has been iterated that there is no global agreement upon the percentage of signet-ring cells that are required to establish the diagnosis of primary signet-ring cell carcinoma of the prostate gland and that 5% of signet-ring cells to 50% of signet-ring cells have been described in the literature related to signet ring cell carcinomas of the prostate gland [5].
The nucleus of the signet-ring cell carcinoma signet-ring cell is said to be displaced as well as indented by a clear mucin filled vacuole and that the vacuole must stain positively on mucin staining [5].
Mucin-negative vacuolated “signet-ring cell-like” adenocarcinoma is more common: [5]
May also be included in many studies.
These tumours usually tend to be high-grade tumours also.
Gleason pattern 4, with ragged infiltration as well as poorly formed glands could simulate scattered signet-ring cells.
Cautery in in trans-urethral resection of prostate (TURP) could cause stromal cell vacuoles [5].
The infiltration pattern of the tumour could be as single cells up to sheets-
This rarely may be associated with mucinous carcinoma of the prostate gland [5].
Gleason pattern 5 by definition – [5]
May be associated with other Gleason patterns which usually tend to be 4 or 5.
Poor response to treatment as well as poor prognosis [5].
Immunohistochemistry staining positive staining for: PSA, and PAP [5].
Urothelial and non-prostate origin signet-ring cell carcinoma primary tumours with extension / metastasis to the prostate gland should be excluded [5].
Mucinous urothelial carcinoma – [5]
With regard to urothelial carcinoma, immunohistochemistry staining study of the tumour does demonstrate tumour cells that exhibit positive staining for HMWCK and CK7/20 with double positivity in most of the cases.
With regard to urothelial carcinoma, immunohistochemistry staining of the tumour does demonstrate tumour cells that exhibit negative staining for PSA and PAP [7].
Nevertheless, some older studies on mucinous urothelial carcinoma had reported some positive staining. [5]
Gastrointestinal tract adenocarcinoma must be ruled out –
Immunohistochemistry staining studies of gastrointestinal tract adenocarcinoma tumour specimens tend to demonstrate tumour cells that exhibit negative staining for PSA and PAP.
It has been documented that immunohistochemistry staining studies do demonstrate positive staining for CDX2 in gastrointestinal primary tumours but also positive staining for CDX2 is also reported in 30% of signet-ring cell carcinomas of the prostate gland [8].
It is important to be mindful of the fact that taking of good detailed history from the patient, the undertaking of endoscopy procedures and utilization of radiology imaging are pivotal to confirming the diagnosis of the tumour.
Some of the possible presentations of primary and metastatic signet-ring cell carcinoma include the following:
Incidental finding. – am individual may undergo trans-urethral resection of prostate (TURP) for severe lower urinary tract symptoms or retention of urine that is provisionally diagnosed as related to benign prostatic hyperplasia and histopathology examination of the resected prostate chips would demonstrate features of signet-ring cell carcinoma.
Lower urinary tract symptoms including:
Diurnal urinary frequency.
Urinary urgency.
Poor / diminished flow of urine
Incomplete emptying of urine.
Intermittent / interrupted flow of urine.
Nocturia.
Haematuria
Raised levels of serum prostate specific antigen (PSA)
Normal serum PSA levels in association with an abnormal digital rectal examination features of abnormality in the prostate gland
Dyspepsia – a history of dyspepsia may be narrated in cases of contemporaneous presence of primary signet-ring cell carcinoma of the stomach in cases of the primary tumour within the stomach with metastasis in the prostate gland or a past history of dyspepsia followed by the undertaking of gastrectomy and detailed history might reveal the diagnosis of signet-ring cell carcinoma of the stomach or a review of the pathology slides of the gastrectomy specimen would demonstrate features of signet-ring cell carcinoma that would mimic the morphology features and the immunohistochemistry staining features of the prostatic specimen.
Rectal mass – In cases of contemporaneous primary signet-ring cell carcinoma of the rectum invading or metastatic to the prostate gland there may be a history of sensation of a mass within the rectum which may be palpable upon digital rectal examination and which would be visible upon proctoscopy and colonoscopy and when biopsied would demonstrate features of a signet-ring cell adenocarcinoma of the rectum.
Rectal bleeding - In cases of contemporaneous primary signet-ring cell carcinoma of the rectum invading or metastatic to the prostate gland there may be a history of rectal bleeding and the rectal tumour may be palpable upon digital rectal examination and which would be visible upon proctoscopy and colonoscopy and when biopsied would demonstrate features of a signet-ring cell adenocarcinoma of the rectum.
Retention of urine – On rare occasions a patient may develop retention of urine which may initially be provisionally diagnosed as representing retention of urine due to benign prostatic hyperplasia or conventional adenocarcinoma of the prostate gland.
Raised levels of serum prostatic-specific antigen.
Normal levels of serum prostate-specific antigen may be found in association with lower urinary tract symptoms.
Enlarged benign feeling prostate upon rectal examination.
Abnormal feeling prostate that may upon rectal examination feel:
Elastic or,
Firm or,
Hard or ,
Nodular.
Loin pain – On rare occasions there may be loin pain if the tumour involves the base of the urinary bladder and obstructs the ureter.
Clinical Examination Findings
The general examination and abdominal examination of majority of patients who have signet-ring cell carcinoma of the prostate gland would be normal but in cases of metastatic signet-ring cell carcinoma of the prostate gland that has developed from a primary signet-ring cell carcinoma of the stomach or a gastrointestinal tract organ which had previously been excised, there would be an abdominal scar from a previous operation.
Enlarged benign feeling prostate gland
Nodular feeling of prostate or a nodule found within the prostate gland upon palpation.
A firm area on the prostate upon digital rectal examination of the prostate gland.
A hard feeling of the prostate gland or a hard area within the prostate gland found upon rectal examination.
An elastic area within the prostate gland found upon digital rectal examination and usually this would be non-tender.
Suprapubic tenderness in cases of acute retention of urine due to primary or metastatic signet-ring cell carcinoma of the prostate gland.
Dullness to percussion in the supra-pubic region on rare occasions of signet-ring cell carcinoma of prostate associated with urinary retention.
A palpable urinary bladder mass on rare occasions of signet-ring cell carcinoma associated with retention of urine.
Laboratory Investigations
Urine
Urinalysis, urine microscopy and culture are general tests that tend to be undertaken in the general assessment of all patients who have primary or metastatic signet-ring cell carcinoma of the prostate gland as part of the general assessment of the patients and generally the results would tend to be normal but if there is any evidence of urinary tract infection, it would be treated appropriately with utilization of appropriate antibiotics based upon the antibiotic sensitivity pattern of the cultured organism.
Hematology Blood Tests
Full blood count and coagulation studies are routine tests that tend to be undertaken as part of the general assessment of patients who have primary and metastatic signet-ring cell carcinoma of the prostate gland and generally the results would tend to be normal but if there is evidence of anaemia, it would be treated accordingly to improve upon the general condition prior to the definitive treatment of the tumour. There may also be anaemia in cases of metastatic signet-ring carcinoma with a contemporaneous primary signet-ring cell carcinoma of the rectum associated with bleeding per rectum.
Biochemistry Blood Tests
Serum urea, estimated glomerular filtration rate (EGFR), renal function test, blood glucose, and liver function tests, as well as serum PSA test are routine tests that tend to be undertaken as part of the general assessment of patients who have primary and metastatic signet-ring cell carcinoma of the prostate gland. The same tests tend to be undertaken as part of the follow-up assessment of patients who have undergone treatment for primary and metastatic signet-ring cell carcinoma of the prostate gland.
Radiology Imaging
Ultrasound Scan
Ultrasound scan of abdomen and pelvis and renal tract is a general radiology imaging assessment that tends to be undertaken on individuals who have primary or metastatic signet-ring cell carcinoma of the prostate gland as part of their initial assessment as well as follow-up assessments which could be done together with chest x-rays but this has been superseded by the undertaking of computed tomography (CT) scan of thorax, abdomen, and pelvis. Ultrasound scan of the abdomen and pelvis would ascertain if there is any metastatic lesion within the liver or not as well as if there are enlarged lymph nodes. The ultrasound scan can also define the size and echogenicity of the prostate gland as well as if there are any areas of the prostate gland and also if there is involvement of the urinary bladder by the tumour or not as well as if there is any hydronephrosis due to obstruction of a ureter, the ultrasound scan would demonstrate it.
Ultrasound-scan-guided biopsy of the prostate is a general way of obtaining specimens for pathology examination in the investigation of cases of raised serum levels of PSA as well as abnormal digital examination prostate features and this would most often reveal features of signet-ring cell carcinoma that would establish the morphology and immunohistochemistry study features of the prostatic tumour that would establish the diagnosis of signet-ring cell carcinoma of the prostate gland.
Computed Tomography (CT) Scan
CT scan of thorax, abdomen, and pelvis is a routine radiology image investigation that tends to be undertaken in the initial staging of individuals who have been diagnosed as having signet-ring cell carcinoma of the prostate gland. If there are any tumours elsewhere, enlarged lymph nodes or metastases anywhere, then the CT scan would demonstrate it. Tumours within the stomach, appendix and gastrointestinal tract would also be confirmed or negated as evidence or no evidence of lesions within the aforementioned sites.
CT scan of thorax, abdomen, and pelvis, is a common radiology imaging assessment that tends to be undertaken as part of the follow-up assessment of individuals who have undergone treatment for signet-ring cell carcinoma whether it was a treated primary or metastatic signet-ring cell carcinoma.
CT scan of prostate gland is a radiology imaging assessment that is undertaken for some patients who have raised serum PSA levels or abnormal digital rectal examination of prostate findings as part of the initial assessment of the features of the prostate gland before biopsies of the prostate gland are undertaken by means of ultrasound-scan-guided biopsies of the prostate gland or CT scan guided template biopsies of the prostate gland and examination of the biopsy specimen would most often lead to the diagnosis of the classical adenocarcinoma of the prostate gland and on rare occasions signet-ring cell carcinoma of the prostate gland.
Magnetic Resonance Imaging (MRI) scan
MRI scan of thorax, abdomen, and pelvis is a routine radiology image investigation that tends to be undertaken in the initial staging of individuals who have been diagnosed as having signet-ring cell carcinoma of the prostate gland. If there are any tumours elsewhere, enlarged lymph nodes or metastases anywhere, then the MRI scan would demonstrate it. Tumours within the stomach, appendix and gastrointestinal tract would also be confirmed or negated as evidence or no evidence of lesions within the aforementioned sites.
MRI scan of thorax, abdomen, and pelvis, is a common radiology imaging assessment that tends to be undertaken as part of the follow-up assessment of individuals who have undergone treatment for signet-ring cell carcinoma whether it was a treated primary or metastatic signet-ring cell carcinoma.
MRI scan of prostate gland is a radiology imaging assessment that is undertaken for some patients who have raised serum PSA levels or abnormal digital rectal examination of prostate findings as part of the initial assessment of the features of the prostate gland before biopsies of the prostate gland are undertaken by means of ultrasound-scan-guided biopsies of the prostate gland or CT scan guided template biopsies of the prostate gland and examination of the biopsy specimen would most often lead to the diagnosis of the classical adenocarcinoma of the prostate gland and on rare occasions signet-ring cell carcinoma of the prostate gland.
MRI scan of the prostate has become a common way of assessing the prostate gland in assessing the features of the prostate in cases of raised serum PSA in highly resourced countries because MRI scan of the prostate does provide more detailed features of the prostate gland in comparison with CT scan and ultrasound scan.
Positron Emission Tomography – Computed Tomography (PET-CT) Scan
PET-CT scan tends to be undertaken in the follow-up assessments of patients who have undergone treatment for primary and metastatic signet-ring cell carcinomas to ascertain if they have developed metastasis or not as well as to ascertain the number and sites of the metastases.
Isotope Bone
Isotope bone scan is a radiology imaging scan that tends to be undertaken to ascertain if an individual who has undergone treatment for signet-ring cell carcinoma who has back pain has developed bone metastasis or not.
Upper Gastrointestinal Endoscopy
Upper gastrointestinal endoscopy forms part of the assessment of patients who have signet-ring cell carcinoma of the prostate if they have or have not got symptoms of dyspepsia to ascertain if there is any lesion within the oesophagus, stomach, or duodenum that could be the site of a primary signet-ring cell carcinoma and when this procedure is undertaken biopsies are taken of any suspicious lesions that are visualized and the specimen would be examined by the pathologist to ascertain if the lesion is a signet-ring cell carcinoma.
Colonoscopy
Colonoscopy forms part of the assessment of patients who have signet-ring cell carcinoma of the prostate if they have or have not got symptoms of change of bowel habit of bleeding per rectum to ascertain if there is any lesion within the rectum or large bowel that could be the site of a primary signet-ring cell carcinoma and when this procedure is undertaken biopsies are taken of any suspicious lesions that are visualized and the specimen would be examined by the pathologist to ascertain if the lesion is a signet-ring cell carcinoma.
Trans-urethral resection of prostate (TURP)
On rare occasions individuals would undergo TURP for severe lower urinary tract symptoms or retention of urine that have been diagnosed as related to benign prostatic hyperplasia but surprisingly pathology examination of the resected prostate chips would demonstrate microscopy histopathology and immunohistochemistry staining features of signet-ring cell carcinoma of the prostate gland.
Treatment of Primary Signet-Ring Cell Carcinoma of the Prostate Gland
It has been iterated that the treatment of primary signet-ring cell carcinoma of the prostate gland tends to be similar to the treatment of the traditional adenocarcinoma of the prostate gland which does include: hormonal treatment, radiotherapy, and surgery [6].
Microscopic Histopathology Examination Features of Primary Signet-Ring Cell Carcinoma of the Prostate Gland [6].
It has been iterated that generally microscopy histopathology examination of primary signet-ring cell carcinomas of the prostate gland tends to demonstrate solid, acinar, single-line patterns as well as that the tumour upon microscopy pathology examination tends to be seen as prostatic tumour that is primarily comprised of tumour cells that contain signet-ring cell pattern and at least 25% of signet-ring cells due to intra-cellular accumulation of mucin that has compressed the nucleus into the shape of a crescent [6].
Immunohistostaining Staining Studies of Primary Signet-Ring Cell Carcinomas of the Prostate Gland.
Positive immunohistochemistry staining [6]
It has been iterated that positive immunohistochemistry staining of signet-ring prostate cancer tumour cells have been reported for the ensuing immunohistochemistry stains:
PSA – positive staining for PSA is stated to have been variable in some studies.
AE1/AE3.
CAM 5.2
Ki-67 with a mean of 8%.
PAS-diastase.
Mucicarmine (50%).
Alcian blue (60%).
Alpha-methyl-acyl coenzyme A racemase (P504S). And
Cytokeratin 5/6.
Negative immunohistochemistry staining [6]
It has been iterated that negative immunohistochemistry staining has been reported in primary signet-ring cell carcinomas of the prostate gland as follows:
Bcl2 (rare positive)
CEA (80%).
Electron Microscopy Examination Features of Primary Signet-Ring Cell Carcinoma of the Prostate Gland [6].
It has been stated that electron microscopy examination of specimens of primary signet-ring cell carcinomas of the prostate gland tends to demonstrate intra-cytoplasmic lumina that are lined by micro-villi [6]
Differential Diagnoses of Primary Signet-Ring Cell Carcinomas of the Prostate Gland
Some of the differential diagnoses of primary signet-ring cell carcinomas of the prostate gland have been summated as follows: [6]
Artifactual changes in lymphocytes pursuant to trans-urethral resection of prostate gland (TURP). [6] – It has been documented that microscopy examination of specimen of the prostate that contains artefactual changes within lymphocytes does not show any classic adenocarcinoma of the prostate gland as well as immunohistochemistry staining studies of the specimen does show cells that exhibit negative staining for mucin, PSA, and PAP [9].
Benign signet-ring cell change - It has been documented that with regard to benign signet-ring cell change of the prostate gland microscopy examination of the specimen of the prostate gland would show no evidence of classic adenocarcinoma of the prostate gland and immunohistochemistry studies of specimen of the prostate would demonstrate prostate cells that exhibit negative staining for mucin, PSA, as well as for PAP [10].
Gastrointestinal primary malignant tumour with metastasis within the prostate gland. – It has been iterated that primary malignant signet-ring cell carcinoma with a metastatic signet-ring component within the prostate gland is much more common in comparison with primary signet-ring cell carcinoma of the prostate gland and that microscopy histopathology examination of a specimen of the prostate gland would not demonstrate any typical adenocarcinoma of the prostate gland and when gastrointestinal work up is undertaking including computed tomography (CT) scan of abdomen and pelvis, colonoscopy and biopsy of any lesion that is found and the specimen is examined under microscopy, esophagogastroduodenoscopy and biopsy of any tumour found is submitted for pathology examination which would demonstrate the primary tumour that would be confirmed based upon negative immunohistochemistry staining of the gastro-intestinal tract tumour for PSA and PAP [6].
Mucinous carcinoma of the prostate gland with signet-ring cells – it has been pointed out that more than 25% of mucinous carcinoma of the prostate gland tends to contain extracellular mucin and less than 25% of the tumour cells do feature signet-ring cells [6].
[B] Miscellaneous Narrations and Discussions from Some Case Reports and Case Studies Related to Sign
Warner et al [1]. reported nine (9) patients who were treated with a diagnosis of primary signet ring cell carcinoma (PSRCC) of the prostate gland who were identified among 29,783 cases of prostate cancer that were evaluated at Mayo Clinic from January 15, 1970, until January 2, 2009. They undertook a PubMed search of the English-language literature that had been published from January 1, 1980, to January 1, 2010, with utilisation of the key words signet ring cell and prostate, which identified 42 cases of signet-ring cell carcinoma of the prostate gland. Warner et al [1]. reviewed those cases, together with the additional 9 cases they had identified that were treated within their institution, and they evaluated the clinical characteristics, histological diagnoses, treatment modalities, and outcomes of the cases. Warner et al [1]. Reported the following:
The mean age at the time of diagnosis of the SRCC of the prostate was 68 years (and the ages at the time of the initial diagnosis of the SRCC of the prostate had ranged between 50 years and 85 years).
The mean prostate-specific antigen level was 95.3 ng/mL (and the serum PSA had ranged between 1.9 ng/mL and 536.0 ng/mL; to convert to the serum PSA results to μg/L, to multiply by 1).
Majority of patients that amounted 66% of the patients had non-stage IV carcinoma, the commonest Gleason sum was 8 which was found in 33% of the cases, and the mean survival of the patients was 29 months.
The presence of a primary signet ring cell carcinoma of the prostate was best confirmed by negative findings on gastrointestinal work-up, a positive stain for prostate-specific acid phosphatase, and negative carcinoembryonic antigen test results.
The lessons that can be learnt from this summation include the following:
The incidence of signet-ring cell carcinoma of the prostate gland among the total cases of conventional adenocarcinoma is low and for this reason, it is important for clinicians and pathologists who have not encountered signet-ring cell carcinoma of the prostate gland should have a high-index of suspicion for the diagnostic of the tumour in order not to underdiagnose signet-ring cell carcinoma of the prostate gland.
Considering that the prognosis of primary signet-ring cell carcinoma of the prostate gland is poor with a mean survival of 29 months, there is an urgent need for urologists, oncologists, as well as pharmacotherapy research workers to undertake further research and trials to identify new chemotherapy medicaments that would effectively and safely destroy signet-ring cell carcinoma tumour cells that would not adversely affect patients that have signet-ring cell carcinoma of the prostate.
There is need for the establishment of a global multi-centre treatment studies on utilization of different treatment options including new chemotherapy medicaments, immunotherapy, radical surgery and radiotherapy for the treatment of signet-ring cell carcinomas of the prostate gland.
Torbenson et al [4]. stated that adenocarcinoma of the prostate gland tant contains a signet ring cell (SRC) component is a rare, ant it is an incompletely characterized variant of prostate cancer which must be differentiated from similar tumours of urinary bladder or stomach origin. In their study, Torbenson et al [4]. utilized mucin and immune-peroxidase stains on formalin-fixed, paraffin-embedded sections from 12 adenocarcinomas of the prostate gland that contained signet-ring cell (SRC) components, with antibodies to prostate-specific antigen (PSA), cytokeratins, MIB-1, bcl-2, c-MET, CD44v6, and CD44v7. They performed a comparison study on six urinary bladder and seven gastric carcinomas that contained signet-ring cells (SRCs). The signet-ring cell (SRC) component of the prostate gland was found to be always associated with the usual high-grade adenocarcinoma. Both components of the prostate carcinoma were upon immunohistochemistry staining positive for PSA, AE1/AE3, and CAM 5.2 (12 cases out of 12 were positive for the three tumour markers) and also exhibited positive staining for MET (in 5 cases out of 9 cases), CD44v6 (in 9 cases of out of 10 cases), and CDv7 (in 9 out of 10 cases). Only rare cells did stain positively for bcl-2 (in 3 cases out of 9 cases). The mean MIB-1 proliferation index of the tumours was 8%. Intracellular mucin was identified (periodic acid-Schiff with diastase pre-digestion (PAS-D) in 9 cases out of 10 cases, mucicarmine in 5 cases out of 10 case, alcian blue in 6 cases out of 10 cases). Urinary bladder and gastric tumours exhibited positive staining for PSA (in 3 cases out of 6 cases and 2 cases out of 7 cases, respectively), with utilization of a polyclonal antibody, and for bcl-2 (in 5 cases out of 6 cases, 2 cases out of 7 cases), c-MET (in 6 cases out of 6 cases, 6 cases out of 7 cases), CD44v6 (in 5 cases out of 6 cases, 6 cases out of 7 cases), and CD44v7 (in 4 cases out of 6 cases, 4 cases out of case7), with mean MIB-1 proliferation indices of 15 and 35%, respectively. All of the tumours exhibited negative staining for cytokeratin 34 beta E12. Torbenson et al [4]. concluded that adenocarcinomas of the prostate gland that contained signet-ring cell (SRC) components are typically accompanied by high-grade adenocarcinoma; are variably positive for mucin, with PAS-D being the most sensitive stain; exhibit positive expression for PSA, cytokeratins, MIB-1, bcl-2, c-MET, and CD44 which is similar to that shown by the high-grade adenocarcinoma components; have a low MIB-1 proliferation index; and are not always distinguishable from signet-ring cell (SRC) components of urinary bladder and stomach carcinomas with any of the above stains, including PSA.
Blas et al [11]. iterated that to their knowledge 157 cases of signet-ring cell carcinoma of the prostate gland had been reported in the literature at the time of publication of their article in 2019. They retrospectively searched in tumour registries from Hospital Aleman de Buenos Aires to identify all cases of prostate cancer that had been diagnosed and treated since 1990. Blas et al [11]. analysed variables that included the following: the age of the patients at the time of their initial diagnosis, the median serum prostate-specific antigen (PSA) level, the stage of the tumour, global survival, among others. Blas et al [11]. reviewed the literature and they compared their findings within their review of the literature with their series of 5 cases that were treated in their establishment. Blas et al [11]. Summated their results as follows:
They had identified 5 cases.
Within their series of cases they had found that the mean age of the five patients was 77.8 years with a standard deviation of 3.2
The serum prostate-specific antigen (PSA) levels had ranged between 10.6 ng/ml and 331 ng/ml and the median serum PSA level was 18 ng/ml.
Three (3) out of five (5) of the patients that amounted to 60% of the patients had localized disease and two (2) out the five (5) patients that amounted to 40% of the cases had distant disease at the time of their initial diagnosis.
The median survival rate of the patients was 23 months.
When they compared their cases with the reported series of cases they had reviewed, they found that their patients were of older age and they had a lower median survival.
Blas et al [11]. Made the ensuing conclusions:
Primary Signet ring cell carcinoma of the prostate gland is a rare and aggressive histological variant of adenocarcinomas of the prostate gland.
Treatment of primary signet-ring cell carcinoma of the prostate gland (PSRCCP) is the same as classical adenocarcinoma of the prostate gland with an emphasis on aggressive multimodal treatment.
Based upon the finding of Blas et al [11]. that primary signet-ring-cell carcinoma of the prostate gland (PSRCCP) is associated with an aggressive biological behaviour and even when the tumours are diagnosed initially as localized tumours, the median survival of the patients, it would be argued that there is an urgent need for the establishment of a global multi-centre trials of various aggressive treatment options as an attempt to improve the survival and quality of life of all individuals who have primary signet-ring cell carcinomas of the prostate including: new treatment options, radical surgery, combination chemotherapy including use of new chemotherapy medicaments, radical radiotherapy, and immunotherapy.
Gök et al [12]. reported a 70-year-old man who manifested with lower urinary tract symptoms and a raised serum PSA level of 7.26 ng/ml. He underwent digital rectal examination which did not demonstrate any hardness or nodules. He underwent a 12-core biopsy of his prostate gland and pathology examination of the biopsy specimen demonstrated features of a Gleason grade 5 + 5 = 10 adenocarcinoma of the prostate gland within all quadrants of the prostate and a signet ring cell component in nearly half of all quadrants examined (see figure 1A). Immunohistochemistry staining studies of the tumour demonstrated negative staining for leukocyte common antigen (LCA) and alfa smooth muscle actin (ASMA), but the tumour cells exhibited positive staining for PSA (see figure 1B) as well as positive staining for prostate specific acid phosphatase (PSAP). Cytoplasmic immunostaining with PSA within the tumour cells did support the origin of prostatic adenocarcinoma. Gök et al [12]. iterated that with regard to their reported case, there was a strong cytoplasmic staining with PSA within signet-ring-like cells. Colonoscopy and endoscopy were undertaken in order to exclude metastasis from the gastrointestinal (GI) tract to the prostate gland in view of thee signet ring cell component of the tumour. Biopsies were obtained from suspicious areas of the gastrointestinal (GI) tract; nevertheless, pathology examination of the biopsy specimen did not demonstrate any evidence of malignancy. Computed tomography (CT) scan of abdomen and pelvis was undertaken to assess the pancreas and other abdominal organs and no pathological signs were found. Additionally, he had whole body bone scintigraphy which also did not identify any metastasis. Based upon the aforementioned findings the patient was diagnosed as having non-metastatic disease. He underwent treatment that consisted of an LHRH analogue (Goserelin acetate, 10.8 mg, subcutaneous) and radiology-image-guided radiotherapy at a daily dose of 200 cGy/fr, 6MV-X-ray beams were utilized, 7200 cGy to prostate, 6600 cGy to vesicula seminalis, 5000 cGy to bilateral pelvic lymph node region were delivered in 34 fractions) was undertaken. His serum PSA level which was 7.26 ng/mL before hormonotherapy decreased to 0.37 ng/mL three months pursuant to the commencement of the hormonal therapy (HT). His serum PSA level which was 0.37 ng/mL before radiotherapy was noted to decrease to 0.32 ng/mL after radiotherapy (RT). The patient had a serum PSA level of 0.12 ng/mL and no evidence of the disease was identified at his16 month’s follow-up assessment after the start of the treatment.

Gök er al [12]. made the ensuing summations related to their review of the literature on signet-ring cell carcinomas of the prostate gland:
The signet ring appearance within the cells does occur in view of the fact that the nucleus is pushed to the periphery of the cell by large intracytoplasmic vacuoles.
SRCC tends to be most commonly observed within the gastrointestinal (GI) tract. Therefore, when SRCC is identified within the prostate gland, endoscopy, colonoscopy and abdominal CT scan would be required to exclude metastasis.
Their reported case did not demonstrate any GI tract pathological signs. Based upon these findings they established the diagnosis of primary prostatic SRCC.
Some studies had iterated that signet ring cells must constitute of at least 20–25% of the tumour in order to be able to make a diagnosis of primary prostatic SRCC, even though other studies had documented that a certain ratio of cells was not needed for diagnosis. [4] [13] [14]. [15]
With regard to their case, the signet ring cell component had constituted almost 50% of the tumour.
It has been iterated that primary prostatic SRCC tends frequently to be accompanied by high grade adenocarcinoma of prostate patterns, therefore it could be a variant of a high-grade adenocarcinoma rather than it being a separate pathological diagnosis [1, 2].
It must not be ignored with the explanation that an appearance similar to signet rings could be formed in smooth muscle cells and lymphocytes of the prostate gland pursuant to needle biopsies and transurethral resections of the prostate gland. In order to exclude such a situation, it has been iterated that it needs to be demonstrated that the sample was not stained with LCA and ASMA in immunohistochemistry staining studies must be undertaken [13].
It has been iterated that immunohistochemistry staining studies do show that primary SRCC of the prostate gland cases are 87% positively stained for PSA/PSAP staining while this cancer is less frequently positive for Periodic acid-schiff (50%), Alcian blue (44%), mucicarmine (40%) as well as Carcinoembryonic antigen (20%) staining [1].
With regard to their reported case, immunohistochemistry staining of the tumour did demonstrate positive staining for PSA and PSAP on the other hand LCA and ASMA staining was negative. With regard to their reported case, the strongly positive staining with PSA in signet-ring-like cells also suggested that the primary origin of the tumour is the prostate tissue.
The results of their review of the literature revealed that the median age for prostatic SRCC is about 68 years, which is comparable to their reported case of 70 years. [1,13].
At the time of diagnosis, majority of the patients that had been reported in the literature had locally advanced or metastatic disease that was associated with a poor disease prognosis [1] [13].
The study by Fujita et al., did find that only the disease stage at the time of diagnosis was associated with the survival, and not serum PSA levels nor applied therapy modalities [13].
Additionally, they did demonstrate that the survival rates after the initial diagnosis was 82.3% within the first year, 54.7% in the third year and 11.7% in the fifth year [13].
Saito et al. demonstrated that only 27.3% of patients who had SRCC of the prostate gland did have a 3-year survival rate, with no survival at 5 years [16].
Warner et al. demonstrated an average survival time of 29 months [1].
In view of the rare frequency of prostate SRCC of the prostate gland, no consensus opinion or standard treatment management option is available.
The literature has shown that most cases of primary SRCCs of the prostate gland have tended to be treated with hormone therapy (HT), radiotherapy (RT) and radical prostatectomy (RP) or combinations of these therapies. [1, 2, 4, 13-16].
One study did report successful result with gastrointestinal (GI) cancer chemotherapy (FOLFOX) [17].
Warner et al. showed the best survival of patients is with HT+RP and HT + RT combinations treatments [1].
Yoshimura et al. reported that patients who had primary SRCC of the prostate gland had survived 100 months after the commencement of hormonal therapy (HT) plus radiotherapy (RT) combination therapy without any evidence of the disease in their control follow-up [18].
Lilleby et al. reported that they achieved local control and remission in one of their patients 12 months after the commencement of hormonal therapy (HT) plus radiotherapy (RT) combination therapy [19].
A study in the Mayo Clinic with 27,983 patients who had been diagnosed as having prostate cancer showed only nine cases with SRCC of the prostate gland [1]. One of these patients was treated with a combination of hormonal therapy (HT) plus radiotherapy (RT) and he had survival without any evidence of disease at during his 4th year follow-up assessment visit [1].
Their reported case also did achieve a survival of 16 months after the commencement of hormonal therapy (HT) plus radiotherapy (RT) combination treatments without any evidence of the disease at his follow-up
Gök et al [12]. made the ensuing conclusions:
No standardized treatment for SRCC of the prostate gland does exist due to the fact that it is a rare disease.
Nevertheless, the adoption of an aggressive multi-modal treatment would seem reasonable in view of the poor prognosis of the disease.
Radiotherapy in combination with hormonal treatment could be an appropriate alternative treatment for SRCC of the prostate gland.
Fujita et al [13]. reported a case of primary signet ring cell carcinoma of the prostate in a 75‐year‐old man. His serum prostate- specific antigen (PSA) level at his presentation was 9.3 ng/ml. The tumour was confined within the right lobe of his prostate gland and he was treated with a combination of neoadjuvant hormonal therapy and radical prostatectomy. At the time of the report of his case, he was alive with no evidence of disease 12 months pursuant to his radical prostatectomy. None of the prostatic tumour was stained with periodic acid‐Schiff and Alcian blue. Immunohistochemistry staining studies of the tumour demonstrated that the tumour cells had exhibited positive staining for PSA and prostatic acid phosphatase and negative staining for carcinoembryonic antigen. The lesson learnt for this case report is that utilization of hormonal treatment of neo-adjuvant hormonal therapy and radical prostatectomy for the treatment of localized primary signet-ring cell carcinoma of the prostate gland could be associated with a good short-term to medium-term outcome but because the case was reported with a short-term follow-up data, one cannot predict the long-term outcome of this patient. Nevertheless, considering the fact that majority of cases of primary signet-ring cell carcinomas that had been reported previously had had a poor outcome with a reasonably short survival, it would be argued that currently and in the future, anyone who is diagnosed as having localized primary signet-ring cell carcinoma should be treated aggressively and if they are fit to undergo surgical operation, then they should be considered for neo-adjuvant hormonal therapy, plus radical prostatectomy, plus combination chemotherapy, plus immunotherapy. Or there should also be the possibility of entering such patient into a global multicentre clinical trial that would include novel treatment options (radiofrequency ablation of tumour / irreversible electroporation, cryotherapy / selective prostatic artery angiography and super-selective embolization of the arterial branch supplying the tumour plus adjuvant therapy (chemotherapy / immunotherapy).
Kim et al [20]. iterated that primary signet ring cell carcinoma (SRCC) of the prostate gland is very rare and that even though signet-ring cell carcinoma (SRCC) tends to be primarily found within the stomach and colon, it could also be found within the pancreas, breast, thyroid, bladder, as well as within the prostate gland. Kim et al [20]. had recently diagnosed and treated a case of primary signet-ring cell carcinoma (SRCC) of the prostate gland. Kim et al [20]. reported a 56-year-old Korean man was referred to their institution for evaluation of a one-month history of haematuria and a recently found urinary bladder mass. He underwent transurethral resection of the urinary bladder tumour (TURBT) and histopathology examination and immunohistochemistry staining studies of the resected tumour specimen demonstrated features that established a diagnosis0 of signet-ring cell carcinoma (SRCC) with tumour invading into the outer half of the deep muscularis propria. Three weeks later, he underwent radical cystoprostatectomy with ileal conduit construction. The tumour was found to have involved both his prostate gland and his urinary bladder, but the centre of the tumour was noted to be located within his prostate gland. He underwent duodenoscopy and colonoscopy both demonstrated no evidence of tumour origin from within the gastrointestinal (GI) tract. Overall, the tumour was regarded as primary signet-ring cell carcinoma (SRCC) of the prostate gland. Concurrent chemoradiotherapy (CCRT) using leucovorin and fluorouracil was initiated two months subsequently. He eventually developed bone and liver metastases and died of hepatopathy. A lesson learnt from this case report is that primary signet-ring cell carcinoma of the prostate gland that has involved the urinary bladder does portend an aggressive biological behaviour and at times aggressive treatment including radical cystoprostatectomy plus radical radiotherapy plus combination chemotherapy may not provide adequate treatment of curative intent and because of this additional treatment including immunotherapy and utilization of more effective combination chemotherapy options that do need to be developed must be utilized.
Kwon et [21]. reported a 61-year-old Korean man, who was referred to their institution because of high level of his serum prostate-specific antigen (PSA) that was recorded as 8.1ng/mL and urinary frequency, as well as nocturia which he had developed over the preceding four (4) months. He had his first trans-rectal ultrasound scan (TRUS)-guided prostate biopsy and pathology examination of the specimen revealed feature of a benign prostatic hyperplasia. About 3 years later, the patient did revisit their institute because of elevated level of his serum PSA that was noted to be 14.7 ng/mL as well as because of back pain. He underwent a second TRUS-guided prostate biopsy. Histopathology examination and immunohistochemical staining studies of the biopsy specimen demonstrated features of a signet ring cell carcinoma (SRCC). Also there was radiology image evidence of multiple bony metastasis. He was commenced on androgen deprivation therapy (ADT). Nine months later, he was diagnosed with hormone refractory prostate cancer and the ADT was changed into docetaxel chemotherapy. The patient died after 2 cycles of chemotherapy. A lesson that was learnt from this summation is the fact that primary signet-ring cell carcinoma of the prostate gland is an aggressive type of tumour that tends to be associated with poor prognosis and death and that hormonal treatment alone would not provide adequate treatment for individuals who develop primary signet-ring cell carcinomas with bone metastases and such patients need to be treated aggressively with a combination of hormonal therapy plus radiotherapy, plus chemotherapy plus immunotherapy. It would also be argued that there is need to develop new and more effective chemotherapy medicaments that would more effectively destroy signet-ring cell carcinoma tumour cells but which would not have any deleterious effect on patients.
Tiwari et al [22]. stated that primary signet-ring cell carcinoma (SRCC) of the prostate gland is a rare clinical entity which tends to be characterised by its aggressive nature and dismal prognosis. Tiwari et al [22]. reported a case of an advanced signet-ring cell carcinoma (SRCC) of the prostate gland that manifested as a large pelvic mass that was associated with obstructive uropathy and rectal involvement which was managed by complete androgen blockade. At his 24 months follow-up, the patient did not have any evidence of progression or metastasis. Tiwari et al [22]. iterated that aggressive management with utilization of multimodality approach with the combination of surgery, radiotherapy and hormonal treatment could emanate in long disease-free survival in some patients, despite the aggressive nature of this disease.
Sungur et al [23]. stated that primary signet-ring cell carcinoma of the prostate (PSRCCP) is a very histological variant of tumour which usually originates from the stomach, colon, and pancreas and primary signet-ring cell carcinoma of the prostate gland (PSRCCP) was first reported in 1979 and there have been case series with small numbers of patients as well as case reports in the literature. Signet-ring cell carcinoma of the prostate gland does have a poor outcome in comparison with the classic adenocarcinoma of the prostate gland. Sungur et al [23]. reported a case of primary signet-ring cell carcinoma of the prostate gland that was treated with maximal androgen deprivation therapy with zoledronic acid. This case report had added to the literature the fact that zoledronic acid is one of the medications that has been used as one additional treatment option for primary signet-ring cell carcinoma of the prostate gland.
Hashimoto et al [24]. in 2017 iterated that signet-ring cell carcinoma (SRCC) of the prostate gland is rare, and approximately 100 case reports had been published up to the time of the report of their case. Hashimoto et al [24]. reported a very aggressive case of signet-ring cell carcinoma (SRCC) of the prostate gland in a Japanese man. The patient did receive estramustine, docetaxel, and carboplatin combination chemotherapy, which was followed by TS-1 and CPT-11 combination therapy. They reported that unfortunately, the disease had progressed, and he died of general metastatic disease which was treated over 16 month with systemic chemotherapy. This case report has demonstrated the aggressive nature of signet-ring cell carcinoma of the prostate and this case report would also highlight the need to develop new treatment options that would effectively and safely destroy signet-ring cell carcinoma tumour cells so as to improve the prognosis of patients who are afflicted by primary signet-ring cell carcinomas as well as improve upon the quality of lives of individual that are afflicted by signet-ring cell carcinoma of the prostate gland.
Ishizu et al [25]. reported a 67-year-old man who had presented with dysuria. His digital rectal examination demonstrated that his prostate gland was enlarged and stony hard. His serum prostate specific antigen level was abnormally high at 46.2 ng/ml. He underwent prostate biopsy and pathology examination of the biopsy specimen demonstrated features that confirmed a diagnosis of signet ring cells which upon immunohistochemistry staining showed tumour cells that were stained positively for prostate specific antigen as well as the pathology examination also demonstrated poorly differentiated adenocarcinoma. He had computed tomographic (CT) scan which did demonstrate enlargement of his para-aortic lymph nodes. He was commenced on endocrine therapy with luteinizing hormone-releasing hormone agonist. After two months, his serum prostate specific antigen level decreased to the normal range. Ishizu et al [25]. stated that the pathological findings and the good response to endocrine therapy in their reported case did suggest that signet ring cell carcinoma of the prostate is only a morphologic variant of ordinary prostatic adenocarcinoma. Despite the opinion of Ishizu et al [25]. it would be argued that this case was reported with a short-term outcome and considering the fact that majority of cases of signet-ring cell carcinomas of the prostate gland have been associated with poor prognosis, there is a high possibility that in the near future, the tumour would become hormone refractory and hence there is need for the establishment of a global multi-centre trial with utilization of various multi-modality treatment options with an aim to provide treatment of curative intent from the onset, rather than wait till the tumour is hormone refractory in the future.
Dols et al [26]. iterated that primary signet-ring cell carcinoma of the prostate gland is not a frequently encountered tumour and even more so as a case of a secondary spread of signet-ring cell carcinoma sub-type from elsewhere into the prostate gland. Dols et al [26]. reported the sixth (6th) case of secondary signet-ring cell carcinoma of the prostate gland secondary to a primary gastric cancer. Five years pursuant to undergoing gastrectomy to resect signet-ring cell carcinoma of the stomach, they identified a secondary intra-prostatic spread of the tumour with urinary obstruction. Upon examination, Dols et al [26]. found out that the physical appearance of the prostatic tumour simulated that of the previously-resected signet-ring cell carcinoma of the stomach. No evidence of metastases to other sites of the body were found upon investigations and the patient underwent radiotherapy. Dols et al [26]. iterated that when confronted with intra-prostatic signet-ring cell adenocarcinoma, it would be necessary to differentiate between primary and secondary aetiology in view of the fact that this would reflect in the choice of treatment and prognosis of the disease. Considering the fact that that this reported case was a metastatic signet-ring cell carcinoma with the primary tumour having originated from a previous signet-ring cell carcinoma, some people would argue that radiotherapy for the metastatic tumour that was localized with the prostate gland would not provide adequate treatment of curative intent even though radiology imaging did give the impression of a localized tumour within the prostate gland but it would be envisaged that there could be microscopic metastatic signet-ring carcinoma cells in other organs of the body and for this reason additional treatment including combination chemotherapy and immunotherapy should be considered in future cases that mimic the reported case so that if there are microscopic tumour cells elsewhere which computed tomography (CT) scan or positron emission tomography – computed tomography (PET-CT) scan cannot detect, then the tumour cells could be effectively destroyed before they develop in the future as aggressive visible tumours that may prove difficult to treat.
Cimino et al [27]. stated that as is well-known, signet ring cell carcinoma (SRCC) rarely does appear as a histopathology finding in the prostatic tissue. However, a differentiation should be made between a primary tumour and a metastatic disease. Cimino et al [27]. reported the case of a 52-year-old man who had lower urinary tract symptoms, total serum PSA of 0.2 ng/ml, elevated serum levels of CEA and CA19-9. Two years preceding his manifestation, he underwent total gastrectomy and pathology examination of the specimen showed features the confirmed the diagnosis of a poor differentiated adenocarcinoma with signet-ring cell component. A palpable nodule within his prostate gland was found upon digital rectal examination and for this reason he underwent 12-core trans-perineal prostate biopsy and pathology examination of the specimen showed features that confirmed a diagnosis of poor differentiated adenocarcinoma with signet-ring cell and adipose tissue infiltration. Immunohistochemistry staining studies of the specimen showed that the tumour cells had exhibited positive staining for PAS, CK7 and CDX-2, focal positive staining for CK20 and-+ negative staining for PSA and PSAP. The diagnosis of a prostatic secondary signet-ring cell carcinoma (SRCC) was considered to be possible given the positivity to CK7, CDX-2, focal positivity to CK20 and negativity to PSA. Cimino et al [27]. concluded that signet-ring cell carcinoma is a rare histological finding in prostate cancer and for this reason it would be necessary to differentiate a primary tumour from a metastatic disease. For these reasons, immunohistochemistry staining studies for CK7, CK20 and CDX-2 would seem to be useful with regard to the diagnosis of the primary site of the tumour
Yoh et al [28]. reported a rare case of primary signet-ring cell carcinoma of the prostate gland (PSRCCPG) in an advanced stage. They reported a 62-year-old man whose serum level of prostate-specific antigen was raised at 364.70 ng/ml and who was diagnosed as having cT4N1M1c signet-ring cell carcinoma of the prostate gland that was classified as Gleason score 5 + 4 = 9. Immunohistochemical examination of specimen of the prostatic tumour demonstrated cytoplasmic immunoreactivity to prostate-specific antigen within the signet-ring cancer cells. The intracytoplasmic vacuoles in the signet-ring cells demonstrated mucin production with a positive staining with periodic acid-Schiff. Even though the patient received hormonal treatment, the disease progressed and lead to his death 15 months after the diagnosis of his signet-ring cell carcinoma of the prostate gland. The lesson learnt from this case report is that primary signet-ring cell carcinoma of the prostate gland is an aggressive malignant tumour that generally tends to be associated with poor prognosis and for majority of these tumours treatment with hormonal therapy alone should not be considered as adequate treatment of curative intent and that it would be argued that all cases of signet-ring cell carcinomas should be treated aggressively with multi-disciplinary team combination treatment approach.
Khan et al [29]. reported a 74-year-old man who had manifested with urinary frequency, dysuria as well as symptoms that were suggestive of lower urinary tract obstruction which he had progressively developed over the preceding 3 months. He was noted to be a smoker, as well as to be an occasional drinker of alcohol. He was asymptomatic otherwise apart from infrequent episodes of dyspepsia. He had trans-rectal ultrasound scan of his prostate gland which demonstrated a Grade III enlargement of his prostate gland that measured 5.5 cm x 4.2 cm x 4.8 cm that was consistent with a 58 grams of prostate gland as well as suspicious hypo-echoic areas within the peripheral zone and a residual urine volume of 80 ml. His total serum PSA level was 9.71 ng/ml and the free-to-total serum PSA ratio was 10.8. He had a rectal examination which demonstrated that his prostate gland was elastic, slightly hard, painless, as well as with prominent retro-prostatic sulci. The results of his routine haematology blood tests demonstrated microcytic hypochromic anaemia as well as an elevated erythrocyte sedimentation rate. He had a chest radiograph which did not reveal any abnormalities. He underwent cystoscopy examination which did not demonstrate any abnormality within his urinary bladder and an extensive trans-urethral resection of his prostate gland (TURP) was undertaken under general anaesthesia with resection of 45 grams of prostate. Histopathology examination of the resected prostatic chips demonstrated nests and singly infiltrating poorly differentiated, hyperchromatic, pleomorphic adenocarcinoma cells and majority of these tumour cells were noted to be of signet-ring cell morphology (see new figure 2 – old figure 1. Figure 3, and figure 4). Additionally histopathology examination of the prostatic tumour specimens showed individual cells and cell nests that were visualized lying haphazardly amongst bundles of smooth muscle fibres as well as within lympho-vascular spaces but there was no evidence of peri-neural invasion, mucinous fibroplasia, or glomerulations found upon the examination. The initial provisional diagnosis that was considered was a variant of invasive adenocarcinoma of the prostate gland with a Gleason score of 4+5=0; nevertheless, immunohistochemistry staining of the specimen for PSA (see figure 4 inset) as Carcinoembryonic Antigen (CEA) were contemporaneously undertaken in view of the fact that primary signet-ring cell carcinoma of the prostate gland is rare and therefore it is mandatory to exclude other mucinous tumours of non-prostate origin based upon the morphology of the tumours and immunohistochemistry staining features of the tumours and if required utilization of clinical information as suggested by Eble et al [30]. The immunohistochemistry staining for both PSA and CEA were negative. The globoid optically clear cytoplasm of the signet-ring cells stained positively with Alcian blue at a PH of 2.5 which did confirm the contents of acid mucin ((see figure 2 (inset)). Two weeks pursuant to undergoing TURP, he underwent upper gastrointestinal endoscopy and biopsy of gastric lesions and histopathology examination of the biopsy specimen demonstrated features of an infiltrating signet-ring cell carcinoma of the stomach. He had computed tomography (CT) scan which demonstrated no evidence of liver metastases and it only demonstrated only enlarged regional lymph nodes. He underwent radical gastrectomy and follow-up chemotherapy was instituted. At his 6-months follow-up pursuant to his initial prostatectomy he was found upon his assessment to be doing well.
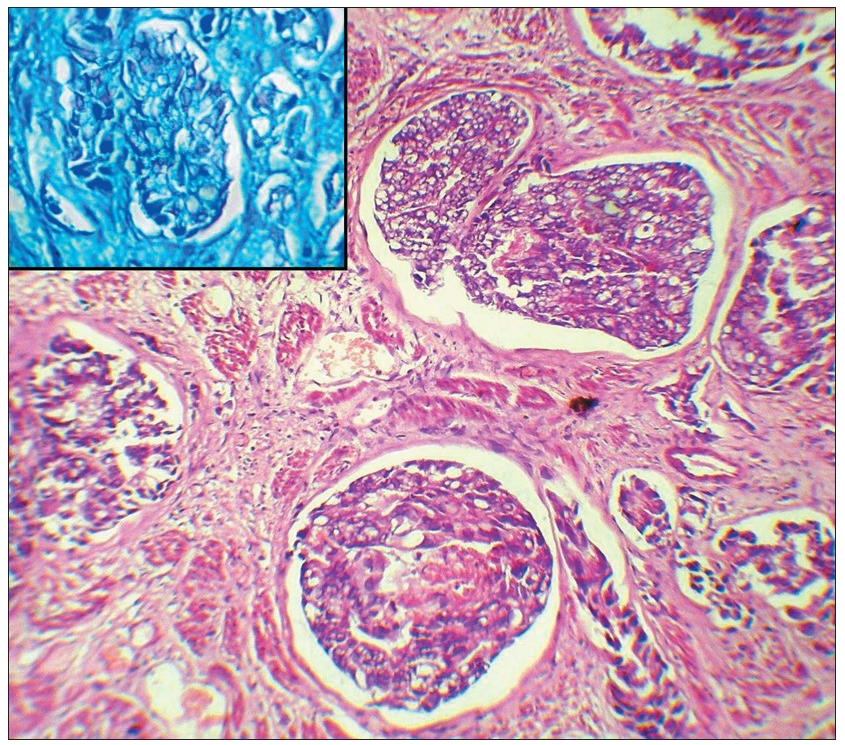
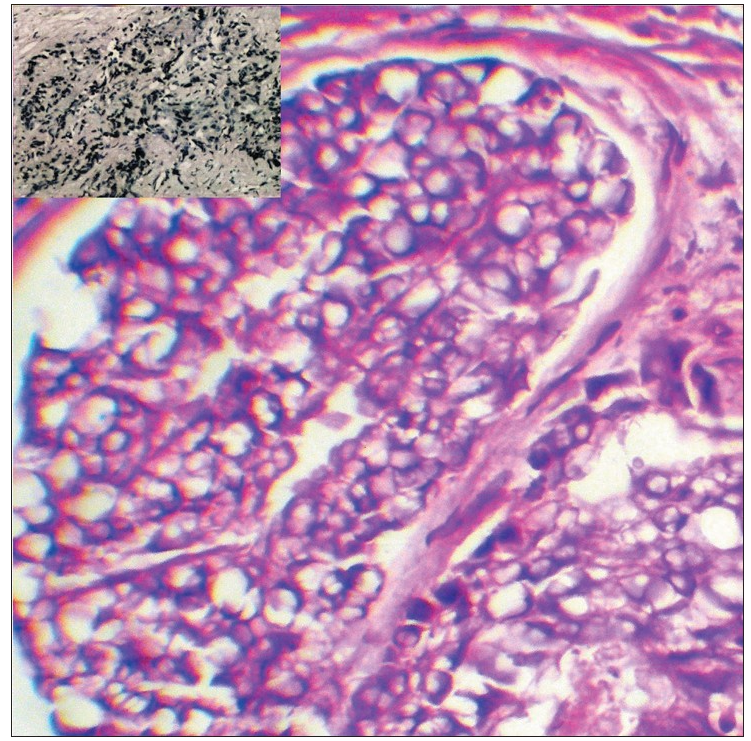
Khan et al [29]. made the ensuing summations related to signet-ring cell carcinomas of the prostate gland and gastrointestinal tract organs:
It has been iterated that some primary adenocarcinomas of the prostate gland would have a signet-ring-cell appearance feature; nevertheless, the vacuoles do not contain intracytoplasmic mucin [15]. These vacuolated cells could be present as singly invasive cells, in single glands, and in sheets.
Some authors had iterated that only a few cases of prostate cancer have been reported that contain mucin positive signet ring cells [31, 32].
It has been advised that clinicians should exclude other mucinous tumours of non-prostatic origin based upon morphology and immunohistochemistry features of the tumours and if necessary with utilization of clinical information [30].
Some authors had iterated that immunohistochemistry staining for PSA is diagnostically helpful with regard to differentiating adenocarcinomas of the prostate gland from other tumours that secondarily involved the prostate gland and establishing prostate origin in metastatic carcinomas of unknown primary [33, 34].
It has also been documented that a minority of higher grade adenocarcinomas of the prostate gland are exhibit negative staining for PSA, even though some of these tumours had been demonstrated to express PSA mRNA and that some adenocarcinomas of the prostate gland do lose PSA immunoreactivity pursuant to androgen deprivation or radiation therapy [30].
It has been stated that with regard to gastric signet ring cell carcinoma (WHO classification) [35] greater than 50% of the tumour does consist of isolated or small groups of malignant cells that contain intracytoplasmic acid mucin which stain with Alcian blue at pH 2.5.
Khan et al [29]. Additionally stated the following:
Their reported case once again has underlined the fact that metastatic signet-ring cell (SRC) carcinoma even though rare, it should be taken into consideration as a differential diagnosis before diagnosing a primary SRC carcinoma of prostate.
A detailed clinical examination and special attention to any antecedent history of mild symptoms like dyspepsia could lead to the performance of an upper gastrointestinal endoscopy which could be helpful with regard to the much earlier detection of a primary gastric tumour.
The most important feature for differentiation with regard to their case that was associated with an occult primary signet-ring ring cell carcinoma was PSA immunostaining of the tumour which was supplemented by an Alcian blue stain at PH 2.5
Signet-ring cell carcinoma of the prostate gland is an uncommon type of tumour that may be occasionally diagnosed as a primary or metastatic cancer which tends to an aggressive tumour that tends to be associated with poor prognosis in comparison with the classic adenocarcinoma of the prostate.
Signet-ring cell carcinoma of the prostate gland could be a tumour that tends to be admixed with adenocarcinoma or other cell types of tumour or it may be a pure tumour.
There is no global consensus opinion regarding what percentage of signet-ring cell carcinoma tumour cells should be in the tumour to enable a firm diagnosis which needs to be clarified by global academic urologists, pathologists, and oncologists in order to clarify the dilemma.
There is no global consensus opinion regarding the best treatment options for primary as well as metastatic signet-ring cell carcinomas of the prostate gland and this needs to be clarified by a consensus global opinion group on signet-ring cell carcinomas of the prostate gland including academic urologists, oncologists, pathologists, and pharmacotherapy research workers.
A multi-centre global trial of various treatment options including novel less-invasive treatments plus neo-adjuvant / adjuvant therapies plus the traditional treatment options of radical prostatectomy, radiotherapy plus various neo-adjuvant and adjuvant therapies should be included in the trials.
Conflict of interest: Nil – I have no conflict of interest to declare.
Journal of Clinical Medicine for granting permission for reproduction of figures and contents of their journal article under the Creative Commons Licence provided the authors, the Journal and the source of the article are properly cited.
Nigerian Journal of Surgery [serial online] for granting permission for reproduction of figures and contents of their Journal article under the Creative Commons Agreement Licence provided the original source is properly cited.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
